


















Last updated: May 2026.
What Are the Highest Paid Medical Specialties in the US? (2026 Data)
Physician compensation in the United States increased by approximately 3% in 2025, bringing the average physician salary to $386,000, according to the Medscape 2026 Physician Compensation Report. That survey covered 5,916 full-time physicians across more than 29 specialties, with data collected between September and December 2025. While 3% growth is modest, it follows a period of rising overhead costs, Medicare reimbursement cuts, and increasing consolidation of physician practices, all of which continue to reshape how doctors are paid and how much they take home.
This updated guide includes the latest statistics across all key categories, from highest-paid medical specialties and regional pay variations to the continued income gap between private practice and employed positions, as well as differences in earnings between MDs and DOs. We have also added updated context on the wRVU system, 2026 Medicare changes (including the first positive conversion factor adjustment in six years), the widening gender pay gap, and the ongoing decline of physician-owned practices.
We have compiled a list of medical specialties in the United States with the highest yearly income. The income data is based on several sources, including the Medscape 2026 Physician Compensation Report, the Doximity 2025 Physician Compensation Report, and additional industry data.
Eight specialties now average more than $500,000 per year, up from four in the prior year’s report. Here are the top-earning specialties based on the most recent available physician compensation data:
| Specialty | Income |
|---|---|
| Orthopedic Surgery | $611,000 |
| Cardiology | $575,000 |
| Radiology | $571,000 |
| Plastic Surgery | $554,000 |
| Anesthesiology | $543,000 |
| Urology | $535,000 |
| Gastroenterology | $530,000 |
| Otolaryngology (ENT) | $508,000 |
| Hematology/Oncology | $462,000 |
| Dermatology | $449,000 |
| General Surgery | $447,000 |
| Critical Care | $424,000 |
| Ophthalmology | $446,000 |
| Pulmonology | $394,000 |
| Pathology | $392,000 |
| Emergency Medicine | $389,000 |
| OB/GYN | $378,000 |
| Nephrology | $360,000 |
| Physical Medicine & Rehab | $351,000 |
| Psychiatry | $335,000 |
| Neurology | $338,000 |
| Allergy & Immunology | $309,000 |
| Internal Medicine | $299,000 |
| Rheumatology | $284,000 |
| Family Medicine | $286,000 |
| Infectious Disease | $282,000 |
| Endocrinology | $284,000 |
| Pediatrics | $266,000 |
| Preventive Medicine | $277,000 |
Key Trends in 2026:
Orthopedic surgeons remain firmly at the top, with average compensation jumping to $611,000.
Eight specialties now cross the $500,000 mark, up from four in the previous year’s report. The new additions above $500K include anesthesiology, urology, gastroenterology, and otolaryngology.
Cardiology saw the highest year-over-year compensation growth at 10%, followed by radiology (9%), ophthalmology (9%), and anesthesiology and orthopedics (both around 8%).
Seven specialties saw pay decreases: physical medicine and rehabilitation, nephrology, dermatology, oncology/hematology, pulmonary medicine, allergy and immunology, and psychiatry all reported slight declines of 1% to 3%.
Primary care specialties continue to lag, with an average of $298,000 compared to $417,000 for specialists.
Pediatrics remains the lowest-compensated major specialty at $266,000, while rheumatology and pediatric compensation held flat from the prior year.
For students interested in understanding how specialty competitiveness relates to these figures, our breakdown of the most competitive medical specialties in the United States provides additional context on match rates, training length, and demand.
How Do Doctors in the United States Get Paid?
Determining and articulating how doctors in the US get paid is almost as difficult as determining how much they earn annually. As we’ve already mentioned, calculating how much a physician earns is dependent on many factors. The healthcare landscape in the United States is constantly changing and evolving due to the introduction of new bills, laws, and other institutional changes.
Let’s review the different factors that affect a doctor’s income.
Private Practice vs. Employed
According to the American Medical Association (AMA), the primary difference in compensation lies in their employment status (employed vs. private practice).
Self-employed physicians continue to outearn employed physicians on average. While exact 2025 income figures for self-employed versus employed physicians have not yet been confirmed in the Medscape 2026 report’s public data, the structural gap remains significant. In prior years, the difference was approximately $38,000 annually, with self-employed physicians averaging roughly $391,000 and employed physicians around $353,000. The underlying reasons for this gap have not changed: practice owners share directly in revenue and can control overhead, scheduling, and payer negotiations in ways that employed physicians cannot.
However, the number of physicians who actually own or co-own a practice continues to shrink. According to the AMA’s 2024 Physician Practice Benchmark Survey (published May 2025), only 42.2% of physicians worked in wholly physician-owned private practices in 2024. That is an 18-percentage-point decline from 60.1% in 2012. Even more striking, only 35.4% of physicians had any ownership stake in their practice, down from 53.2% in 2012.
The share of physicians working in practices with 10 or fewer physicians has now dipped below 50% for the first time in the survey’s history, falling from 61.4% in 2012 to 47.4% in 2024. Meanwhile, the percentage of physicians working in hospital-owned practices increased from 23.4% in 2012 to 34.5% in 2024, and the percentage working as a direct hospital employee or contractor rose from 5.6% to 12.2% over the same period.
Similar to any business owner, self-employed doctors determine their income after accounting for expenses. Patients visit the office, are seen, and the practice bills patients or insurance companies for services rendered. For example, if a doctor’s office generates $350,000 in revenue and invests $200,000 in running the business (rent, supplies, salaries), that leaves approximately $150,000 to be divided among owners. Actual figures will vary widely by specialty, location, practice size, and payer mix.
It is in the best interest of a private practice to serve as many patients as possible per day. The revenue of the business heavily depends on how many patients they see and bill each day. If the number of patients decreases, so does the revenue.
In recent years, private practices have become less common among physicians in the United States. Per the most recent AMA data, only 42.2% of doctors in America remain in a private practice setting. When asked why, physicians overwhelmingly pointed to payment and financial issues along with complex bureaucracy and regulatory demands. Over 70% of physicians whose practices were sold said that the need to “better negotiate higher payment rates with payers” was either “very important” or “important” in motivating the sale, according to the AMA.
Hospital systems, private equity firms, and corporate entities are acquiring more practices. As of 2022, approximately 4.5% of physicians worked in a practice owned by a private equity group, and 38% of those in PE-owned practices said they had been acquired in the past five years. Many doctors report that this consolidation trend is driven by administrative burdens, challenges with insurance negotiations, and interest in steady income.
As with any business, running a private practice is no easy task. Many doctors grow tired and frustrated with the regulations and responsibilities of managing such an enterprise. On top of dealing with rent and employees, they have to deal with insurance companies, Medicare, and malpractice insurance. For many doctors, being an employee of a hospital or other medical facility provides peace of mind and a stable income. Even though employed doctors are expected to demonstrate a high productivity level, their income is not solely reliant on their productivity.
This is not overly simplistic, though. Hospitals within the United States have created protections for reduced physician productivity. Many hospitals throughout the US have created pay packages for their physicians. These pay packages reward physicians who put in hard work. The work relative value unit, commonly referred to as the wRVU, is a system that attempts to reward and compensate doctors for demonstrated enthusiasm and extra work, like seeing additional patients. In this aspect, the revenue model and income of private practices are also present in larger medical institutions. The more patients a doctor serves, the higher they are paid.
wRVUs and Productivity-Based Pay: Work Relative Value Units (wRVUs) remain the dominant structure for productivity bonuses in 2026. According to the Medscape 2026 report, RVUs continue to be “by far the most common way of calculating these bonuses.” Data from SullivanCotter indicates that physician productivity has largely stabilized, with wRVU output increasing about 1.5% overall year over year. Compensation per wRVU ratios have also normalized, suggesting that recent pay gains are driven more by market pressure and labor competition than by increased output. While there was a push toward quality-based bonuses in prior years, productivity volume remains the primary driver of physician pay in most settings.
Many healthcare systems in the US are looking to change their pay structure to adapt to certain rules put in place by Medicare. However, it is hard to imagine that the US healthcare system would move away from rewarding physicians based on the number of patients they serve. A lot of attention is being paid to both the quality and efficiency, meaning the value of the care will consider more than the number of patients served. As one can imagine, it is hard to find the right balance between the two. With all business models, pay in the healthcare industry is reliant on productivity, but the shift in the structure of healthcare compensation seeks to align productivity and quality of care.
Medicare Reimbursement: A Turning Point in 2026
For the first time in six years, Medicare’s Physician Fee Schedule conversion factor is going up. CMS finalized two conversion factors for 2026: $33.57 per RVU for services furnished by Qualifying APM Participants, and $33.40 per RVU for all other services. These represent increases of 3.77% and 3.26% respectively over the 2025 conversion factor of $32.35.
The increase is largely attributable to a one-time 2.5% boost to the conversion factor included in the “One Big Beautiful Bill Act (H.R. 1),” which Congress passed in early July 2025. This reversal is significant: adjusted for inflation in practice costs, Medicare physician payment had declined 33% from 2001 to 2025, according to AMA analysis. Whether this single adjustment signals a sustained trend or a one-time correction remains to be seen.
However, the 2026 fee schedule also introduces a new wrinkle. CMS is applying a “efficiency adjustment” of -2.5% to work relative value units (wRVUs) for many procedural, non-time-based services. The practical effect is that while the conversion factor rises, the wRVU values assigned to many surgical and procedural codes are being reduced. This appears to advance CMS’s stated goal of increasing reimbursement for cognitive specialties (such as primary care) while offsetting those increases through reductions in procedural specialty payments. For physicians in high-volume surgical practices, the net effect of these changes will depend on their specific procedure mix.
Income Difference by Region and State
The state and region in which a doctor practices also affects their income. Many would think that states with larger populations would have higher incomes among doctors, but this is not the case. Surprisingly, heavily populated states like California and New York do not consistently rank among the top-earning states for physicians. This may come down to several factors. Large, economically developed states have an abundance of healthcare options, meaning patients have many choices when it comes to selecting a healthcare provider. This means that, on average, there are fewer patients per doctor within these states. As previously discussed, the United States healthcare system is structured around earnings based on how many patients one serves. Fewer patients per doctor means less income, which is likely why large, populated states have lower-earning doctors.
States in the Midwest and Southeast have historically been among the top-earning regions for physicians overall. In these areas, healthcare options can be more limited, meaning there are not as many doctors, hospitals, or other medical facilities. This correlates to there being more patients per doctor. In general, physicians who practice in states with lower populations tend to fare better in terms of income than those who practice in large, populated states with an abundance of healthcare options.
According to the Medscape 2026 report, average physician pay varies by region as follows:
| Region | Average Income/Physician (2026) |
|---|---|
| Midwest | $400,000 |
| West | $390,000 |
| South | $381,000 |
| Northeast | $375,000 |
The Midwest has led regional physician compensation for two consecutive years, with an average of $400,000 in 2025 (up from $385,000 the year before). Physicians in high-cost-of-living states in the Northeast often earn less than counterparts in Midwestern and Southern states, largely due to higher overhead, different payer mixes, and greater competition among providers.
If you are interested in how physician demand varies not just by state but by country, our article on which country has the highest demand for doctors offers a broader perspective on global workforce needs.
Income Difference by Specialty
Primary care practitioners earn an average of $298,000, while specialists earn around $417,000, according to the Medscape 2026 report. These are estimated averages based on recent survey data and may vary significantly depending on factors like individual practice setting, experience, and location. We’ve provided a list of the top-earning medical specialties within the US, which you can reference at the beginning of the article.
Remember, these are estimates, and individual income can vary greatly.
Why does a specialty affect a doctor’s income? To put it simply, some specialties require more training and involve higher-acuity procedures than others. For example, medical specialties such as cardiology, orthopedics, and plastic surgery are some of the top paid within the United States. All of these specialties are procedure-based and require five to six years of additional residency training after graduating from medical school. The specialties mentioned also tend to demand post-residency, sub-specialty training such as fellowships. If you are considering whether additional graduate study might help strengthen your application, our article on whether grad school helps you get into medical school addresses that question directly.
Primary care specialties like family medicine, pediatrics, and internal medicine require less training. Aspiring physicians can become family physicians after six years of education (four years of medical school and two years of residency). While physicians practicing in these specialties earn less, there is an upside. The upside being they have a smaller debt and can enter the workforce quicker by spending less time and money on specialty training. They also accrue less debt because they can begin paying off their school debt quicker.
When it comes to choosing a specialty, you should consider the demand for that specialty within the health field. Often, higher-earning specialties are more in demand, as an increase in earnings often foreshadows a shortage in that field. Students pursuing PA careers will find a parallel pattern; our breakdown of the highest paid specialties for physician assistants shows similar trends in how procedural and surgical PA roles command higher pay.
MD vs. DO Salary
We cannot avoid mentioning the salary difference between MD vs. DO physicians. DO and MD physicians make comparable income when working within the same specialty; however, specialty options have historically been more limited for DO physicians. Per the latest data from the Main Residency Match, MD and DO graduates are now nearly equally competitive overall. In the 2026 Main Residency Match, U.S. MD seniors achieved a PGY-1 match rate of 93.5%, while U.S. DO seniors achieved 93.2%, their highest on record. The gap between the two is now just 0.3 percentage points.
However, DOs are still less represented within the most lucrative surgical specialties. While the DO match rate has improved dramatically since the merger of MD and DO residency accreditation under the ACGME, competitive specialties like orthopedic surgery and dermatology continue to have lower DO representation.
Although there is a discrepancy within the numbers, there has been a large increase in DO representation in competitive surgical residencies. This is primarily due to the changes in the accreditation of residency programs. Osteopathic and allopathic residencies used to be accredited by different institutions: the former by the AOA and the latter by the ACGME. Now, MD and DO programs are accredited by the ACGME, giving osteopathic programs the same status as allopathic programs. The same accreditation allows DOs to participate in MD programs and allows MDs to partake in programs with “Osteopathic Recognition” designation.
The now unified accreditation is closing the gap between MD and DO residents. Over time, the difference in numbers between the two will likely shrink. However, it is important to remember what DO stands for. DOs have a philosophy that leads them to pursue primary care and non-intrusive medical care practices. DOs are capable of becoming surgeons, but their tenets still affect their career choices, such as specialty and where they practice. For more on the differences between the two degrees, see our article on what DO means after a doctor’s name.
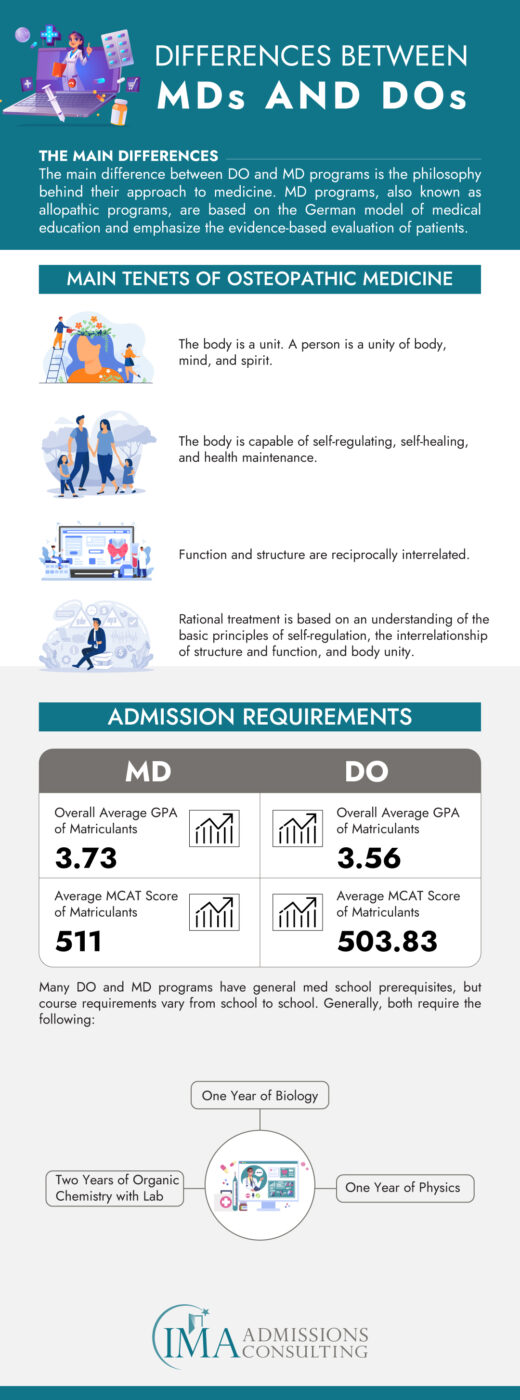
For those deciding between becoming an MD physician or a DO physician, it is best to evaluate both programs as a whole rather than based on potential income. Keep in mind that when working in the same specialty, DOs and MDs earn roughly the same annual income. However, there are many factors to consider when choosing between a DO and MD program. First, one must consider the philosophy of both programs and determine which best aligns with their personal values. You should also consider what medical specialty you’d like to practice. As mentioned, DOs have less representation within surgical specialties, so while this doesn’t mean you can’t be a DO and work within a surgical specialty, it may be easier to get into your preferred specialty as an MD.
MD vs. DO Salary Comparison
The degree alone (MD or DO) does not affect income, but specialty distribution does. On average, based on the most recent earnings data:
MDs earn about $400,000 annually.
DOs earn around $350,000 annually.
This difference is primarily because MDs are more frequently represented in high-paying surgical and procedural specialties. When DOs and MDs work within the same specialty, studies consistently show that their salaries are virtually identical. Employers do not typically differentiate pay based on the physician’s degree type; compensation is based on the role, responsibilities, and clinical performance.
Residency Match 2026 Data:
MD PGY-1 match rate: 93.5%
DO PGY-1 match rate: 93.2% (a new record high, with 8,503 active applicants)
The DO-MD match rate gap has essentially closed. A 0.3 percentage point difference is the smallest in the history of the unified match. However, DOs remain underrepresented in several competitive specialties. In contrast, DOs continue to be well represented in family medicine and primary care, where compensation is lower but entry is more accessible.
Shift Toward Value-Based Care
Although value-based care is a priority for Medicare and some private payers, fee-for-service remains the norm in 2026. Physicians are still mostly compensated based on volume, meaning the number of patients seen or procedures performed.
Models like bundled payments, shared savings programs, and quality score-based bonuses are in use, but not yet widespread enough to dominate physician compensation. For most doctors, productivity (measured in wRVUs) remains the primary determinant of pay. The 2026 Medicare fee schedule does signal CMS’s continued interest in shifting value toward cognitive services and primary care, but whether this translates to meaningful changes in private-payer contracts remains uncertain.
The Gender Pay Gap in Medicine: 2026 Data
One of the most significant findings in the Medscape 2026 Physician Compensation Report is the widening gender pay gap. Average pay among male physicians in 2025 was $429,000, compared to $327,000 for female physicians. The resulting 31% gap is the largest in the survey’s history, up from 29% in 2023.
The Doximity 2025 report, which used a different methodology and adjusted for specialty, location, and years of experience, found a 26% gender pay gap, with women physicians earning an average of $120,917 less than men. Notably, average compensation for men rose 5.7% in 2024, compared with just 1.7% for women, meaning the gap is actively widening rather than closing.
Multiple factors contribute to this disparity. Women remain more concentrated in lower-paying specialties like pediatrics and family medicine. They are also more likely to work part-time or in academic settings, which tend to offer lower compensation than private practice. However, research consistently shows that even when adjusting for specialty, hours worked, and experience, a meaningful gap persists. This is a systemic issue that the profession continues to grapple with.
Racial and Ethnic Pay Disparities
The Medscape 2026 report also highlighted compensation differences along racial and ethnic lines. Physicians identifying as white reported 6.1% higher compensation on average ($391,000) than Asian American physicians ($383,000), Latino physicians ($361,000), and Black physicians ($342,000). These disparities reflect a combination of factors including specialty distribution, practice setting, geographic location, and systemic barriers to career advancement. While compensation reporting by race and ethnicity is still relatively new in these surveys, the data underscores that pay equity in medicine is not solely a gender issue.
Physician Workforce Strain and Satisfaction
Compensation figures tell only part of the story. According to the Medscape 2026 survey, 53% of physicians said they feel fairly compensated individually, up from 48% the year before (which had been the lowest level in a decade of Medscape surveys). However, 61% said they believe the medical profession overall is underpaid.
These feelings are not without basis. The Doximity 2025 report found that the majority of physicians surveyed reported being overworked, with more than two-thirds either looking for an employment change or considering early retirement. In Medscape’s survey, 40% of physicians said they found time and opportunity to take on paid work outside their regular working hours, which can be read as either a sign of entrepreneurial drive or economic necessity.
For pre-med students and those early in their training, these workforce realities are worth understanding. They are not reasons to avoid medicine, but they do mean that choosing a specialty, practice setting, and location should involve more than comparing salary tables. Factors like workload sustainability, administrative burden, and practice autonomy matter enormously to long-term career satisfaction.
Economic Impact of Medical Specialties on Healthcare Systems
In analyzing the economics of healthcare systems, the financial trajectories of medical specialties are not isolated figures. They reflect broader economic currents within the medical industry. High-earning specialties often indicate areas where patient demand intersects with complex, resource-intensive procedures. For instance, specialties like orthopedics and cardiology involve advanced surgical procedures and ongoing care, which typically incur higher costs and, consequently, higher revenue streams for healthcare facilities.
The financial health of hospitals and clinics is inextricably linked to the services provided by these high-earning specialties. These departments can be significant profit centers, helping to subsidize other vital but less lucrative areas of care. For example, a hospital’s state-of-the-art cardiology wing can fund community health initiatives or undercompensated care that benefits the broader population.
Concentration of High-Earning Specialties
Furthermore, the concentration of high-earning specialties has implications for healthcare accessibility. Regions with a higher density of well-compensated specialties may attract more medical talent, which can improve local healthcare services’ quality and availability. Areas predominantly served by lower-earning primary care providers may struggle with attracting and retaining physicians, impacting patient access to specialized care.
The cost of care is another aspect influenced by the distribution of medical specialties. High-earning specialties often require significant investment in technology, facilities, and staff training. While they bring in substantial revenue, they also contribute to the rising costs of healthcare for patients and insurance providers. This raises questions about the sustainability of current healthcare models and the potential need for reform, particularly in how medical services are valued and reimbursed.
The remuneration associated with various medical specialties is not merely a reflection of individual doctors’ income potential. It embodies complex dynamics within healthcare economics, affecting everything from hospital operations and healthcare accessibility to the overall cost of medical services. A nuanced understanding of these dynamics is crucial for stakeholders at all levels, from policymakers and healthcare administrators to medical professionals shaping their career paths.
Value-Based Care: Progress and Resistance
The healthcare industry has been in a prolonged transition from a volume-based to a value-based care model. This shift is intended to reshape not only healthcare delivery but also the financial incentives that underpin the medical profession. The volume-based system, which rewards the quantity of services provided, is slowly giving way to a model that prioritizes the quality of patient outcomes and the efficiency with which care is delivered. However, as of 2026, fee-for-service remains dominant in practice, even as policy language increasingly favors value-based approaches.
This movement towards value-based care is driven by the need to curtail rising healthcare costs while improving the standard of care. In the value-based framework, physicians and hospitals are compensated for helping keep people healthy and for improving the health of those with chronic conditions in cost-effective ways. This model can potentially de-incentivize unnecessary procedures and tests, which can sometimes be a byproduct of the fee-for-service models where healthcare providers are paid for each treatment, scan, or test.
For high-earning specialties, the implications are multifaceted. On the one hand, specialties known for high-intervention procedures, such as orthopedics and cardiology, may see a shift in their income structure. Where previously the income was directly proportional to the number of procedures performed, value-based models may require these specialists to demonstrate that such procedures are not just medically necessary, but also cost-effective and beneficial in terms of patient outcomes. The 2026 Medicare fee schedule’s new efficiency adjustment to procedural wRVUs is one concrete step in this direction.
Value-Based Care Model and Comprehensive Care Coordination
Moreover, the value-based care model emphasizes comprehensive care coordination, which can impact how specialists collaborate with primary care physicians and other healthcare providers. In this context, high-earning specialists will likely need to establish more integrated relationships with other practitioners, ensuring that patient care is optimized across the continuum, from prevention to intervention and chronic disease management.
However, the shift to value-based care also presents opportunities for specialists. Those who can adapt by focusing on patient outcomes and cost-effectiveness may find themselves at the forefront of an industry trend. For instance, orthopedic surgeons who adopt less invasive, patient-centered approaches that demonstrate faster recovery times and lower complication rates may be well-positioned in a value-based landscape. Similarly, cardiologists who integrate lifestyle intervention and medical management to reduce hospital readmissions for heart failure could be seen as models for value-based care.
The transition also has implications for how high-earning specialists negotiate contracts with payers. As value-based metrics become more prominent, these specialists will need to understand and engage with new performance indicators and reimbursement models. This includes bundled payments, where providers receive a single payment for all the services needed to treat a particular condition or care episode, and shared savings programs, where providers are rewarded for reducing healthcare costs while meeting quality benchmarks.
Adapting to value-based care requires not only clinical and operational changes but also a cultural shift within practices and healthcare systems. High-earning specialists must embrace a patient-centric approach that values long-term outcomes over immediate volume. This involves investing in health IT systems for better data tracking and patient engagement, rethinking care pathways to focus on prevention and patient education, and adopting a more collaborative mindset.
The shift towards value-based care is a clear signal that healthcare is evolving, and with it, the financial models that have traditionally defined physician income. For high-earning specialists, the change is both a challenge and an opportunity to redefine their roles within a system increasingly focused on value over volume.
The Role of Medical Education in Specialty Choice
The trajectory of a medical career and the eventual specialty choice a physician makes are heavily influenced by the medical education they receive. The journey to becoming a high-earning medical specialist starts in the lecture halls and clinical rotations of medical schools, where future physicians’ aspirations take shape.
Medical schools play a pivotal role in specialty selection. The exposure students receive to various specialties can significantly sway their career choices. Schools that offer extensive rotations and electives in high-earning specialties like orthopedics or cardiology provide students with insights into these fields, potentially increasing their interest in pursuing them. Conversely, if a medical school emphasizes primary care in its curriculum, students may be more inclined to consider specialties like family medicine or pediatrics. Some students have begun questioning whether the ranking of their medical school affects their specialty options; while name recognition can play a role, clinical performance and board scores tend to matter more.
Educational debt is another crucial factor influencing specialty choice. With the cost of medical education soaring, the debt burden upon graduation can be overwhelming. For many students, this financial pressure nudges them toward higher-paying specialties to manage and eventually pay off their debts. This economic reality can skew the distribution of specialists, with more new doctors gravitating towards lucrative fields and away from less remunerative, yet equally essential, primary care roles. Some students are now considering three-year medical school programs as a way to reduce both time and cost.
The imbalance created by this migration towards high-paying specialties is not without consequences. It can lead to a shortage of primary care physicians, which is already a pressing issue in many parts of the United States. This shortage can compromise the accessibility and quality of healthcare, particularly in rural and underserved urban areas where primary care services are most needed.
What This Means for Pre-Med Students and Future Physicians
Choosing a specialty, state to practice in, and employment status solely based on how much money you may earn is not wise. Money alone cannot sustain one’s passion and dedication for their chosen career. In many ways, your personality and experiences will determine both your specialty and employment status. Some enjoy the autonomy of owning a private practice, while others prefer the steady income and stability offered by being employed at a medical facility.
Although it is difficult to make precise calculations about what the highest paid medical specialties or highest paid doctors are, there is no doubt that some physicians and specialties are among the top earning in the United States. When considering a doctor’s income, it is crucial to consider how long it takes to become a doctor. Earning a medical degree is a huge investment of one’s time, money, efforts, and mental health. The majority of physicians continue paying off their medical school debts long after they have graduated and begun their careers.
In addition to the debt one takes on, the vocation of a physician is not for the faint of heart. The career involves duties and responsibilities many cannot fathom. While there are a considerable number of challenges associated with becoming a physician, one of the latest surveys done by Medscape shows that 77% of polled physicians would choose a career in medicine again if they were still deciding on their future career path.
The 2026 data also tells a more nuanced story than simple salary rankings. The widening gender pay gap, the continued decline of private practice ownership, and the growing share of physicians reporting burnout and considering early retirement all point to a profession under real pressure. For students thinking about medicine, these realities should inform your planning. Understanding how reimbursement works, how practice settings differ, and what drives long-term career satisfaction is just as important as knowing which specialty pays the most.
For those of you who feel you may need additional guidance when it comes to choosing a medical specialty, we recommend seeking the assistance of residency admissions consulting. In addition to admissions consulting, taking part in a medical internship abroad may also aid in making a career path decision. The healthcare internships offered by IMA are a great opportunity to gain structured clinical exposure in a variety of medical specialties, from cardiology and general surgery to pediatrics and internal medicine, while working alongside physicians in real clinical settings.
Frequently Asked Questions
What are the highest paid doctors in the United States?
As of 2026, orthopedic surgeons remain the highest-paid medical professionals in the United States, with an average annual compensation of approximately $611,000 according to the Medscape 2026 report. The Doximity 2025 report, which uses a different methodology, places orthopedic surgery compensation at approximately $679,517. Regardless of the source, orthopedic surgery consistently ranks at or near the top of the physician salary spectrum.
It’s important to note that physician salaries can vary significantly based on factors such as geographic location, years of experience, subspecialty, and practice setting. For instance, orthopedic surgeons specializing in areas like spine surgery or hand surgery may command even higher compensation due to the complexity and demand of these subspecialties. Additionally, physicians practicing in Midwestern states tend to earn higher compensation on average.
Overall, while orthopedic surgery is a highly compensated field, individual earnings are influenced by a combination of personal and professional factors.
What affects a doctor’s income in the US?
The primary factor that affects a doctor’s income in the United States is their employment status. Whether they are self-employed and own a private practice or are employed by a hospital or other medical facility matters significantly. Other factors, such as the doctor’s specialty, affect their income as well. On average, surgical and procedural specialties are among the highest paid doctors in the US, while primary care is among the lowest paid. The region in which a physician practices also affects their income; Midwest physicians currently earn the most on average at $400,000, while those in the Northeast earn the least at $375,000. Gender and race also correlate with compensation differences, with male and white physicians earning more on average.
How do doctors in the United States get paid?
When it comes to getting paid as a doctor in the US, your pay primarily depends on your employment status. If you choose to become a self-employed doctor and run a private practice, your income will be heavily dependent on how many patients you serve. While the productivity of employed physicians is a factor in their salaries as well, it is not as large a factor as it is for self-employed doctors. Doctors employed by hospitals and medical centers have a more stable, steady income. In both cases, the wRVU system remains the most common basis for calculating productivity-based bonuses and compensation adjustments.
Why do doctors in the primary care field get paid less?
Although primary care physicians typically see and serve more patients than other specialized physicians, they typically charge less for their services. This reduced charge stems from the primary care field requiring less training and education than other specialties. In the United States, becoming a family medicine physician requires around six to seven years of education (four years of medical school and two to three years of residency), while it takes nine to ten years to become a doctor in a surgical specialty. Surgical specialties require extra skill and training, and therefore, the services of these physicians end up costing more than those of a primary care doctor. Additionally, procedural services have historically been assigned higher wRVU values than cognitive services, though recent Medicare fee schedule changes in 2026 are beginning to address this imbalance.
Are there any advantages monetarily to becoming a primary care physician vs. a specialist?
Yes, it is true that specialists earn more. They also tend to accrue higher amounts of debt, spending both more time and money on their education. We are not here to dissuade anyone from becoming a specialist. However, money should not be the sole reason you choose to go into a medical specialty. Primary care physicians earn less but have less medical school debt due to graduating sooner and getting out into the workforce quicker. Those within the primary care field, such as family medicine physicians, spend roughly six years receiving their education as opposed to specialists who often spend ten years receiving theirs. Less time spent in medical school equates to less debt and being able to earn money sooner. Simply put, many of the highest paid doctors also have a high amount of medical school debt.
If you feel you may need additional guidance on choosing the best medical specialty for you, consider seeking the professional help of residency admissions consulting or partaking in one of IMA’s pre-med shadowing study abroad programs.
Is there an income difference between MD and DO physicians?
Yes, there is an average income difference between DOs and MDs in the United States, but this difference is largely a reflection of specialty distribution rather than degree-based pay discrimination.
Based on the most recent earnings data, MDs reported an average annual income of approximately $400,000, while DOs averaged closer to $350,000. This roughly 14% gap can appear significant at first glance, but it’s important to understand what’s behind the numbers.
DOs are statistically more likely to enter primary care specialties, such as family medicine, internal medicine, and pediatrics, which tend to have lower compensation. In contrast, MDs are more commonly represented in surgical and high-paying procedural specialties like orthopedics, cardiology, and radiology. These specialties not only require longer post-medical school training but also carry higher reimbursement rates.
When DOs and MDs work within the same specialty, studies consistently show that their salaries are virtually identical. Employers do not typically differentiate pay based on the physician’s degree type; compensation is based on the role, responsibilities, and clinical performance.
In the 2026 Main Residency Match, the PGY-1 match rate gap between U.S. MD seniors (93.5%) and U.S. DO seniors (93.2%) was just 0.3 percentage points, the smallest difference on record. As more DOs enter competitive specialties, a trend that has been accelerating since the merger of MD and DO residency accreditation, this income gap is expected to narrow further.





